
 How does someone know how aerobically fit they actually are? How do you determine if your aerobic program is helping to improve your fitness? Does having a better aerobic fitness level improve your health? Follow along to find out these answers! Being aerobically ‘fit’ or as ‘fit’ as someone can be is a widely accepted goal that everyone should be working towards and is something that is expressed by general practitioners regularly. Being aerobically fit is not just for people who play sports, enjoy running or cycling. People who are more physically active throughout their day or have a more active job also have a higher aerobic fitness. We know this because we can measure aerobic fitness or aerobic capacity and find out the Vo2 max of someone.  What is Vo2 max Vo2 max refers to the amount of oxygen one can bring in, transport and use during a single minute of maximal exertion. Knowing this helps to determine how one's heart, lungs, blood vessels and muscle cells work together. Oxygen is used by the body even at rest, but add in movement and the body starts to use more and more oxygen with increasing intensity. Oxygen is needed at rest because it is used in the production of energy the body needs to survive. When exercising or movement beyond resting the body needs more energy and therefore more oxygen, as the intensity of exercise increases the amount of energy production increases and, you guessed it, the amount of oxygen needed increases. Vo2 max is a way of measuring the body's ability to use oxygen and is measured while exercising when the oxygen demand is the highest, at high intensity. Vo2 Max is referred to as the measure of aerobic capacity or cardio-respiratory fitness.  Why is a good Vo2 max important? It has been widely researched that cardio-respiratory is linked with health and particular cardiovascular disease. In fact, low cardio-respiratory fitness is associated with 2-5x greater risk of cardiovascular disease or all-cause mortality, independent of other cardiovascular disease risk factors. That to me is a very motivating factor behind keeping fit. What is a good Vo2 max? Vo2 max is expressed as either an absolute number or a relative number. The absolute number does not take into account a person's size and while the relative number does. It is hard to compare absolute Vo2 max as everyone is different and everyone weighs differently. Most of the time Vo2 max will be expressed as a relative value which is in ml/kg/min. This means relative Vo2 max will give you the amount of oxygen, in milliliters, you can bring in and utilise per kg of body weight per minute. The following guidelines are taken from the American College of Sports Medicine. These guidelines help compare and understand where someone's aerobic capacity may be as compared to the age and gender. 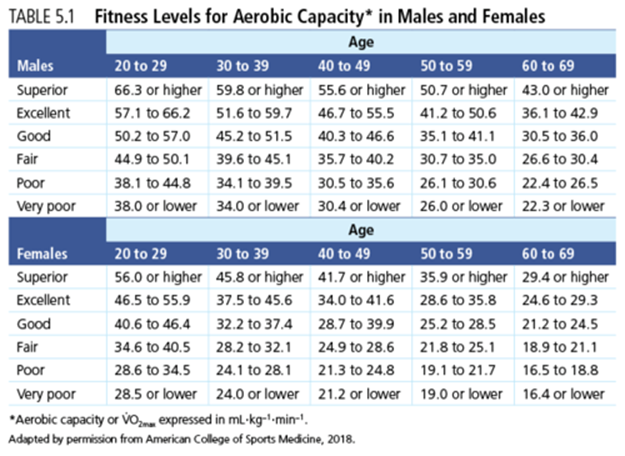 How to measure it The most accurate measurement for Vo2 max is completed in a laboratory where gas analysis is available. To measure Vo2 max using gas analysis, a graded exercise test (GXT) is completed. During the test a subject will ride on a bike or walk/run on a treadmill at increasing intensity, the intensity will increase every 2-3 minutes. Gas analysis is used to accurately measure the amount of oxygen inhaled vs the amount of oxygen and carbon dioxide exhaled while completing the test. The test is completed when maximal oxygen uptake is achieved.  Here in the clinic we don't have gas analysis so, to find out someone's aerobic capacity (Vo2 max) we use a treadmill/bike test where a subject will walk/run/ride while increasing the intensity every 1-3 minutes. During the test we monitor heart rate, rate of perceived exertion and the given workload. The test can be completed to a maximal effort or to a sub maximal effort depending on the subject. From the data we receive we can accurately measure Vo2 max using data driven equations from the American College of Sports Medicine. From this method we can then individualise our aerobic programs to suit exactly the level of the subject which then helps to directly improve their health. If you have any questions pop up throughout this blog please don't hesitate to ask. Izaac Boylan Accredited Exercise Physiologist
0 Comments
 An ACL injury can be a really horrible injury and happens a lot in contact ball sports but can also happen not participating in sport. After an ACL injury more than likely you would go see a doctor ( maybe a sports doctor) and there is a good chance he will do some tests on you around your knee to inform the course of action from there. If there is a suspected ACL injury you will be sent for some imaging to confirm the doctor's thoughts. There is more than one course of action for you to take and this is dependent on your goals and what you want to get back too, this is for you and your doctor/surgeon to discuss. We now know that an ACL reconstruction immediately following an ACL injury does not necessarily mean a better outcome furthermore surgery may not be the answer in individual cases as a favourable outcome can be achieved without surgery. Not to mention the option or ability to have surgery after trying rehabilitation alone first. As EP’s we can work with physios and the treating doctor or surgeon to provide care and a path for rehabilitation back to what you love doing! What is the ACL and ACL injury? The ACL is a ligament in the knee that provides crucial stability to the knee joint. As seen in the picture below it is in the middle of the knee attaching from the thigh bone to the shinbone. The ACL prevents the shinbone from moving forward on the thigh bone. An ACL injury is a tear/rupture or strain of the ligament from some form of forceful impact that strains the ACL more than its current capacity. 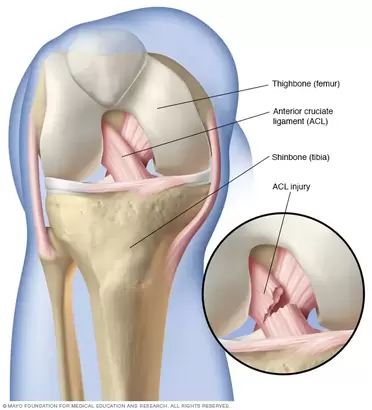 Other injuries commonly happen with an ACL injury, some examples of these may be meniscus injuries, trauma to cartilage, some bone trauma, injuries to other ligaments and some trauma to the joint capsule itself. These other injuries also affect injury prognosis and rehabilitation. Rehabilitation A major factor in ACL rehabilitation is that the process should be outcome based, rather than time based. This means the progression should be based on achieving outcomes that we understand mean readiness for the next phase. This means that specific and valid outcome measures are being used to track progress and guide rehabilitation. Furthermore the program for rehabilitation should be specific to the injured person, everyone's injury is different, everyone responds differently to treatment and everyone has different goals they want to achieve following injury or surgery.  Phases of ACL rehabilitation There are 5 phases of general ACL rehabilitation:
Returning to sport? A more sport specific rehab protocol is the Melbourne ACL Rehabilitation Guide 2.0, this protocol was created by specialist sports physiotherapists that have worked with Olympic teams and elite AFL, netball, soccer and rugby teams, they also do research in the knee rehabilitation space. This guide is very specific and is outcome based and can be tailored to individuals and their goals. The Melbourne ACL Rehabilitation Guide 2.0 is similar to your general ACL rehab however they have included a return to sport phase which essentially assesses your readiness to return to sport both physically and psychologically. The phases are: Pre op, Phase 1 - Recovery from surgery, Phase 2 - Strength and neuromuscular control, Phase 3: Running Agility and landings, Phase 4: Return to sport, Phase 5: Prevention of reinjury. When is the best time to see an Exercise Physiologist (EP)?  Well technically speaking you can begin rehab with an EP for the initial phases of treatment and throughout the whole rehabilitation process. This should be dependent on the experience of the EP dealing with ACL’s and known knee injuries.
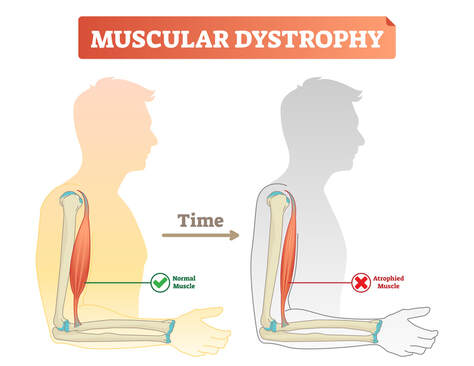
However I would suggest seeing a physio for the early phases of rehab as generally they have more experience around ACL and acute knee injuries as acute muscle and joint injuries is what they specialise in. The best time to see an EP I feel would be either at the intermediate phase or the late phase of rehab, or somewhere in between. EP’s are well equipped to apply principles that govern strength and conditioning and apply these to rehabilitation as this is an EP’s role in musculoskeletal conditions or injuries. After all, the late phase and prevention phases of ACL rehabilitation are primarily strength and conditioning. This would all depend on the individual and the treating physiotherapists preference. All I will say is make sure you are getting sufficiently challenged and measured throughout the entire process and in particular the late stages. ACL rehabilitation is a long process, a long wait to get back to sport or the activity you enjoy! So make sure the process is worth it, you minimise any complications and reduce the risk of a re - rupture! If you need any help with your rehabilitation or want to know more please ask! Izaac Boylan Accredited Exercise Physiologist.  What is Muscular Dystrophy? Muscular dystrophy (MD) is a collection of diseases that cause progressize loss of muscle mass and weakness. It occurs when mutated, abnormal genes disrupt the production of dystrophin, a protein that is needed to build muscle tissue. There are many different forms of MD and unfortunately there are no known cures. The main symptom that is present across all forms of MD is muscle loss and weakness over time, although the age and specific muscle groups this begins in, varies greatly. There are several types of MD, but the most common is Duchenne Muscular Dystrophy, it occurs predominantly in males and symptom onset will usually begin in early childhood. The most common symptoms include;
Effects of Muscular Dystrophy It has been reported that people with MD lose 11-55% of their muscular strength, when compared to those without MD. As the essential protein Dystrophin is absent, it means that muscle tissue cannot repair itself to rebuild, having severe consequences on their overall health long term. Some of these long term effects can include;
 How can exercise help?
Exercise is an effective and accessible treatment option for people with MD. Tailored and specific exercise prescription is safe and can help to counteract muscle loss through increased strength and muscle mass. This assists in delaying the progression of MD and maintaining independence and physical function long term. Exercise has been shown to; increase joint stability, coordination, balance, muscular strength and endurance, fatigue levels, quality of life and mental health. It is recommended to seek exercise therapy as early as possible once diagnosed with MD. What type of exercise is best? For aerobic based exercise low impact and low intensity forms are best. This could include gentle walking, cycling or swimming, focusing on keeping them at a low-intensity level. To use a simple guide, if completing aerobic exercise with MD you should be able to hold a conversation without becoming breathless, if you are not able to, you are most likely working too hard. For strength training low load and high repetition should be the focus, starting small and very gradually building up. As muscle mass and strength will not increase at the same rate as those without MD it is important to not overdo it with strength training. Stretching is also beneficial for maintaining joint range of movement and preventing stiffness. Being mindful to not over extend through a stretch as this with MD can be hypermobile in some joints due to the lack of muscle mass surrounding them and adapted movement patterns. If you have difficulty stretching, having someone assist you with these movements can also be beneficial. If you would like more information about exercising with Muscular Dystrophy or to chat about seeing one of our Exercise Physiologists, please get in touch at info@optimumep.com.au Written By, Aleisha Michael Accredited Exercise Physiologist.  Pain education is a widely used treatment tool in the management of a variety of painful conditions. Education can be used to address some of the commonly held misconceptions around pain and can also be a helpful tool to help someone in pain understand why therapies such as exercise are suitable and recommended for painful conditions. I have touched on this subject in previous blogs however I have recently completed another course in pain management and thought I should spread the knowledge, because after all knowledge is power (and very important - see below) Pain education has grown and changed and is becoming more frequently used. While pain education is an important tool to use to combat persistent pain conditions, a more important factor for recovery is the learning and understanding taking place. Let me explain. 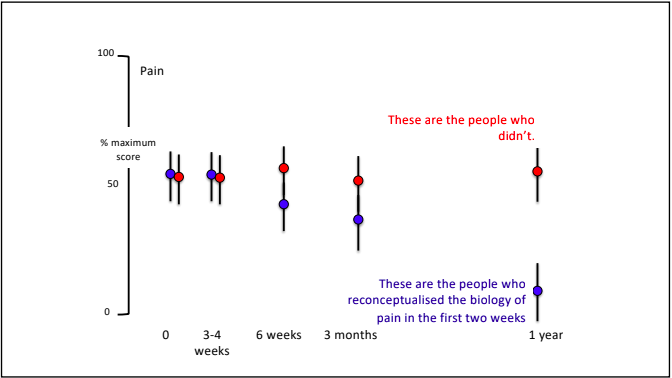 Lorimer mosley’s slides, master sessions, 2022 See the above graph. In this study a group of people with persistent pain underwent pain education. These people were split into two groups which were; Blue - these people were able to understand the biology of pain in the first 2 weeks. And Red - These people were not able to. Effectively the groups were people who were able to learn and understand pain and the people who weren't. As you can see in the graph, at the 1 year follow up, the blue group ( people who were able to understand pain) significantly decreased their rating of pain. This tells us that even though both groups had the same pain education, it was the understanding and learning that was the critical factor in people reducing their pain. I believe in my own experience with low back pain that learning and understanding pain while going through university helped me to recover from the chronic pain I was having. What are the important things to learn to help improve this understanding? To answer this question, it is important to get the perspective of those who have real life experience of persistent pain conditions and were able to recover. Those people were asked following recovery from persistent pain states; “What do you think was the most important information for you to learn to help you recover?” Based on the answers to this question 4 essential facts were created. I have another blog talking through separate facts which are essentially squeezed into these 4 concepts. Fact 1: Pain protects us and promotes healing Pain is fundamentally a mechanism used for protection of the body. Pain is used by the body to prevent injury or damage through behaviour change. Think of pain as the body’s alarm system. If the body is in danger of injury or harm, pain will be used as a protective mechanism to stop whatever you are doing to prevent any harm. If an injury occurs, then the body will sensitise the area of injury to prevent further harm. This means pain will be felt long before there is any potential injury or harm and this allows the body to heal. Therefore pain is protecting us and promoting healing. Once the body heals, it becomes less sensitive and we can go back to normal. Pretty clever hey. Follow the video for a short explanation for what we mean by, pain protects us and promotes healing. Fact 2: Persistent pain overprotects us and prevents recovery Although pain is there to protect and help recovery from injury, unfortunately like everything sometimes it does not work the way it was intended. The sensitivity increases or remains after the injury has healed and the effectiveness of the way the body produces pain gets better during persistent pain states. This means that pain may continue after the tissue healing process has occurred. The body learns how to produce pain by strengthening neural pathways and the body is still trying to protect itself even after the injury has recovered. Why the body is still trying to protect itself is different in each and every individual and could include multiple and many reasons. Fact 3: Many factors influence pain Pain originally was thought to be just neural pathways that responded to nerve endings in the tissues of the body. When in contrast we now know that pain is an output produced by the brain which is a result of multiple different influences. The slide below shows the old view vs the new view of pain which shows just how complex pain is! 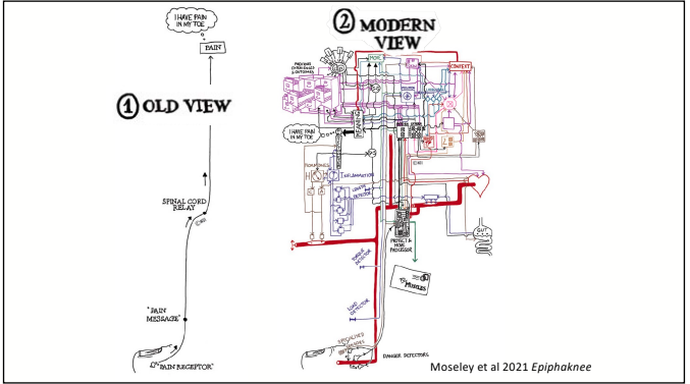 Detection from the tissues in the body plays a vital role in the pain system but new research now tells us that it is neither essential nor necessary for pain to be produced. This means that feeling down, believing you should be in pain or getting told a awful story of someone who had back pain like your own can change the way the pain feels. Now. I'm not saying this is the reason for your pain but I am saying pain is individual and felt different by everyone because everyone has different contextual factors. Things that influence pain can be broken down into 5 categories;
Facts 4: There are many ways to reduce pain and promote recovery. Here is the great part. Now we know pain is influenced by a vast amount of factors, we have a larger amount of things we can target. Of course tissue health plays an important role but potentially your current health is not promoting a great environment for your body, maybe you believe the pain is with you forever and there is nothing you can do about it, or perhaps you are dwelling on past injuries and you are trying to relate those injuries with your current pain. Whatever may be influencing your pain we can target to try to promote recovery. 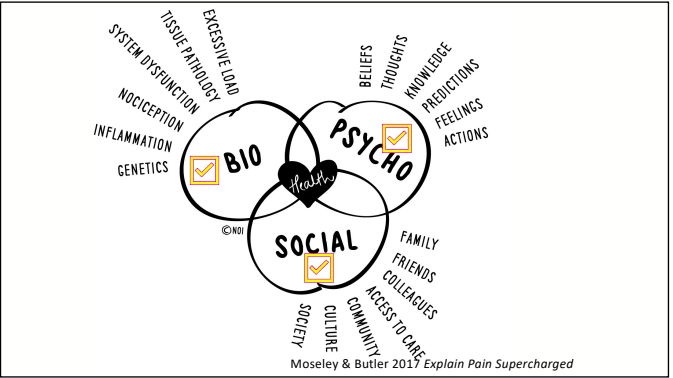 Pain is so very complex and individual to everyone. Learning and understanding this is an important part of not just recovery but any future painful problems.
To start, have an open mind, put in some effort to learn and understand, and seek advice from your trusted evidence based practitioner. Pain is very rarely a quick fix but a journey, more than likely there will be flare ups, but that does not mean you can't move forward again. If you have any questions, please don't hesitate to ask. Izaac Boylan Accredited Exercise Physiologist  Each and every birth is different which also means each Mother’s return to exercise and postnatal recovery will be different too. It is important to check in with your health professional before returning to exercise, ideally this would be a women’s health physio. How long should I wait? There is no one rule that fits all in this circumstance but the general guidelines will differ significantly depending on what type of birth you have. It also depends on what your exercise levels were before giving birth. Vaginal Birth: It is safe to start doing very gentle pelvic floor exercises and slow walks a few days after birth, although more vigorous based exercise should be avoided until after your 6 week check up. Once cleared to resume exercise you should not be exercising at full, pre-birth intensities until around 16 weeks postpartum. Caesarean Birth: As a Caesarean is a major operation it will take at least 6 weeks for tissues to heal. Gentle pelvic floor exercises can be done a few days after birth but gentle low impact aerobic exercise should be done 6-8 weeks postpartum. High impact exercise and heavy weights should be avoided until 3-4 months postpartum once scar tissue has fully healed. Why is exercise beneficial for new Mum’s? Whilst everyone benefits from regular exercise there are some additional benefits for new Mum’s, which include but are not limited too;
What pregnancy changes might affect my ability to exercise postpartum? The female body is amazing and goes through many changes over the course of pregnancy, birth and postpartum. During pregnancy and labour our hormone levels are at an all time high and this can affect your joints and ligaments for up to 6 months afterwards. This highlights why it is important to ease back into exercise even if you are feeling great. During your pregnancy your abdominal muscles may have separated causing Diastus Recti. This can have long term effects if not treated correctly in its early stages and will determine what types of exercises are safe to be doing. The Pelvic Floor is made up of muscles and ligaments that support the bladder, uterus and bowel. This can be weakened during labour, particularly if you had a vaginal birth. Regular pelvic floor exercise can help to strengthen the area and prevent prolapse and leaky bladder in the future. 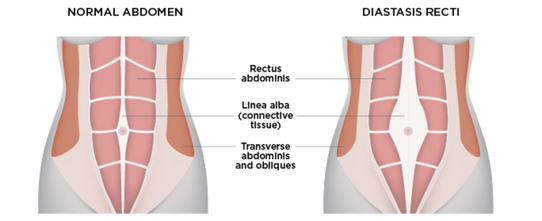 What type of exercise should I be doing?
Low impact exercise will be the best place to start postpartum. In the first few days after birth, focusing on resting and caring for your newborn baby is most important. Some gentle pelvic floor exercises can be done. Think about Squeezing and lifting the muscles around your Vagina as you are trying to hold in a wee, try holding this for 5-8 seconds and then fully relax. Other low-impact exercises that maye suitable include;
Try starting small by incorporating short bouts of exercise into your day. For example walk with the pram down to the shops, think about doing your pelvic floor exercises whilst feeding your baby, etc. Before returning to any exercise postpartum it is important to consult your health professional first and go at your own pace. Written by, Aleisha Michael Accredited Exercise Physiologist. 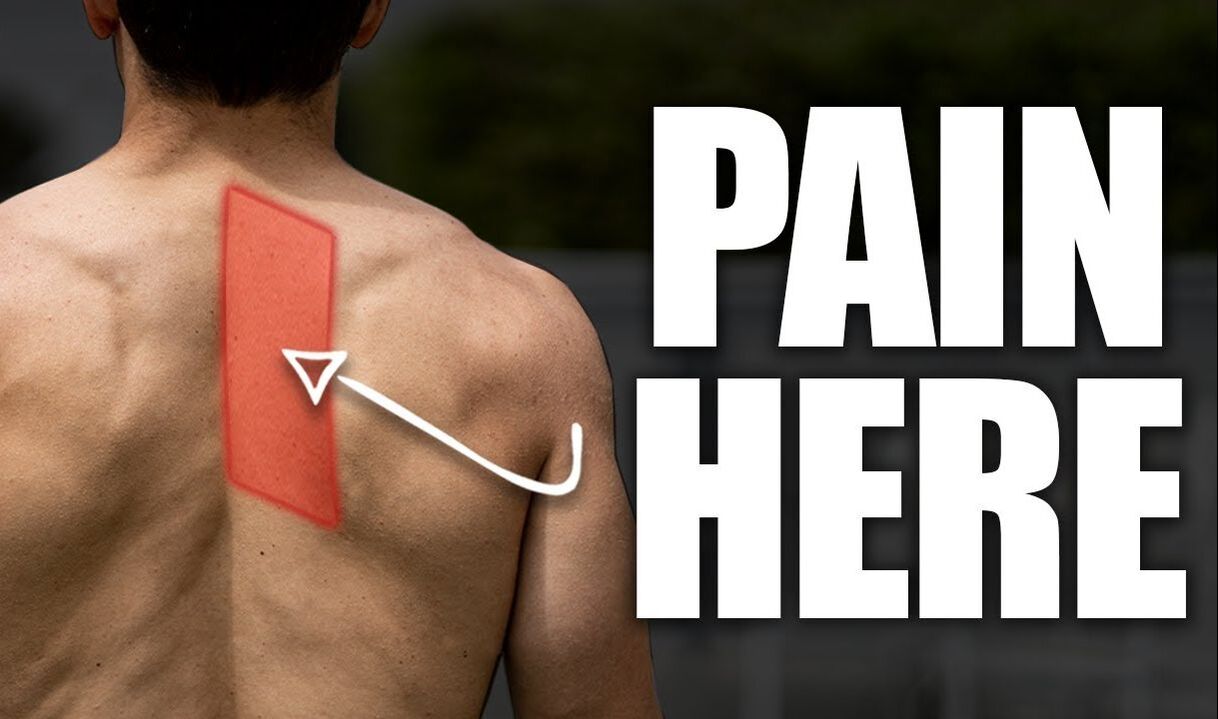 Do you, or have you ever experienced a niggling pain between your shoulder blades and spine? It can potentially reoccur frequently and last a few days or may be more persistent. Whatever the presentation I'm not here to tell you what the cause is because the bottom line is there could be multiple reasons why you have this pain. I’m here to try and give you an understanding of what are the potential causing factors and some strategies to address this. What muscles are near this area? 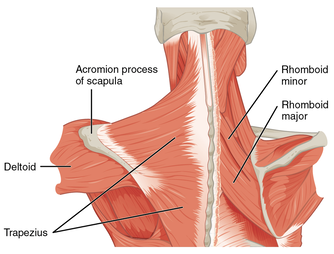 Pain in this region may be called rhomboid pain, the reason being is because both rhomboid minor and major live here (refer to the above image). Both the rhomboid muscles originate on the spine and insert on the medial border of the scapula (inside edge of the shoulder blade). The action of the rhomboids is to retract the scapula (bring the shoulder blades together) and downwards rotate the scapula (like when you bring the arm down from an overhead position). The trapezius muscle is another in this area and is closer to the skin than the rhomboids (see picture above). These two muscles, along with many others, help to move the scapula with the arm to allow for efficient movement when performing your daily task or exercise. 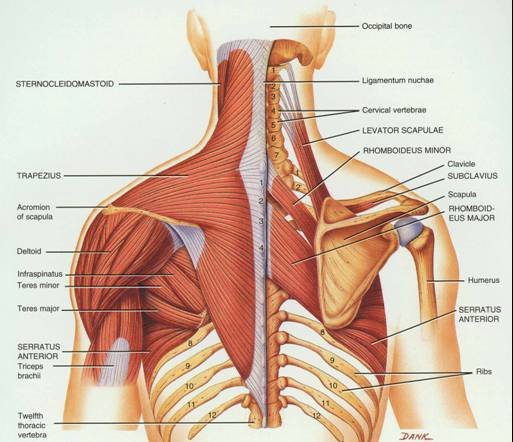 Let's not point the finger too soon. The body moves with an interplay of different systems and structures which rely on each other for efficient movement. When a change to a system or structure happens it may create a problem for another close by in the body. Just because the pain is in between the spine and the shoulder blade, does not mean the rhomboids are the reason for your pain, and even if the rhomboids are in pain they may not be the cause. The body moves with an interplay of different systems and structures which rely on each other for efficient movement. When a change to a system or structure happens it may create a problem for another close by in the body. Let's have a look at what other structures are in the same area or close by including:
It is a bit overwhelming when you look at a picture such as above of just the bones and muscles in this area. However, although there are a large number of potential causes and contributors, we know that improving thoracic mobility can help to improve this nagging pain in your back. Therefore, without being able to individualise a treatment plan on a blog I thought I would give you some exercises to try out! Focusing on thoracic mobility and optimising ( if we know what optimal is) shoulder blade movement. Exercises promoting thoracic mobility Mobility means the ability of a joint to move or be moved freely and easily. With that being said, the thoracic spine is made to be able to move in all different directions, so we need to help it move in all different directions! Two movements that people may tend to require more work in are rotation and extension. Thoracic Rotation Thoracic Extension Excuse my poor thoracic extension!! Exercise promoting shoulder blade movement Movement of the shoulder blade depends on a variety of muscles and although it is unclear what the role of shoulder blade movement on pain and dysfunction is, we can't deny getting the shoulder blade moving and allowing each muscle to do their job is going to be of benefit. One particular muscle that you may benefit from getting moving is the serratus anterior, which lies between the shoulder blade and the rib cage and is responsible for upward rotation (helping the shoulder blade move when you put your arm over head) and protraction (moving your shoulder blades away from each other). Helping the serratus anterior Some tips to remember
If you have this mid back pain, the bottom line is to keep moving! We want to be more mobile and want to minimise the time you sit in one posture. Movement is medicine! Remember this is just general advice! If you are after something more specific Come in and see one of our Exercise Physiologists. Izaac Boylan Accredited Exercise Physiologist  COVID-19 is becoming increasingly prevalent both within our local community and the broader population and it is more than likely at this stage that either you or someone you know has contracted the virus. Find out everything you need to know about returning to exercise after a bout of COVID-19. So... How can COVID-19 affect my ability to exercise? Everyone has different experiences after contracting COVID-19 and this can all be related to your age, gender, overall health and symptom severity. You may initially experience symptoms such as a persistent cough, shortness of breath, fatigue, headaches, body aches, nausea or a sore throat, all of which will impact your ability to exercise. Furthermore if you experience “long-COVID” where symptoms persist for several weeks after having the virus, you may present with inflamed lungs causing significant shortness of breath or high levels of fatigue. These will both limit your physical function and capacity to complete moderate to vigorous intensity exercise. Should I exercise if I have COVID-19? The short answer is no. Research completed by the World Health Organisation tells us that up to 40% of people who contract COVID-19 will be asymptomatic and generally feel fine. If this is the case the recommendation is to complete light movement such as gentle walking or stretching but to avoid moderate to vigorous exercise. For those who do display symptoms of COVID-19 and feel unwell it is advised to rest, increase fluids and complete very gentle movement as even a short walk down the hallway can aggravate shortness of breath in some people. How long should I wait before returning to exercise? There is no one size fits all in regards to this question as recovery from COVID-19 will look different for everyone. Initially being cautious not to spread the virus to others when in the acute stage and presenting with symptoms. This means staying away from gyms, group exercise classes or team sports. Start small and gradually build up, try to think of any daily movement as a form of exercise and increase from there. For example doing a few walks up and down the hallway and stopping once you begin to feel uncomfortable. Exercise has been shown to increase stimulation of the immune system, assisting you to recover from COVID-19. Although be-mindful that mild symptoms can persist up to 6 weeks so it is important to listen to your body and rest when needed, when returning to exercise.  How will I know if I am doing too much? It is important to listen to your body and be aware of what are “normal” signs and symptoms when exercising and what are not. For example it is “normal” to have some degree of shortness of breath and fatigue when exercising. It is NOT normal to have these symptoms when doing gentle, everyday activities that you could previously do with ease. The amount of time you had off from your regular exercise routine is also important to consider. After any period off from our regular exercise routine we need to regress exercises to adjust for our decreased strength and cardiovascular endurance. This may involve reducing the time or distance that you are completing during your cardio or the weight, repetitions or number of sets during strength based exercises. Lastly monitoring your symptoms after exercise and the next day will guide you in knowing if you are doing too much and need to slow down a little bit or if your body is responding well to your volume of exercise. If you are recovering from COVID-19 and not sure where to start when getting back into exercise, one of our Exercise Physiologists can assist you in this process, in a safe and individualised manner. Written by,
Aleisha Michael Accredited Exercise Physiologist  Chronic low back pain is one of the leading causes of disability across the world, not just in Australia. Some people with low back pain are able to live a relatively normal lifestyle which is not influenced to a great degree, however there are many others that have disabling back pain. Disabling back pain can stop sufferers from working, playing with their kids, going on social outings, playing sport, exercising and in severe cases stopping them from being able to perform their daily living tasks. There are a lot of misconceptions or myths around back pain that have become widely thought and used in the management of back pain. These myths and misconceptions may actually hinder your management and progression out of back pain.  In 2019 a group of researchers and Physiotherapists found that they were seeing clients with already strong beliefs around back pain that were not factually correct. They continuously found these common misconceptions and wondered why there was such a gap between clinical practice or common knowledge and what the research says about back pain. Therefore they set out to write 10 facts about back pain backed by research to address the most common misconceptions. Underneath I have outlined the 10 facts about back pain they have discussed in the scientific paper they have published. Fact number 1: Persistent back pain can be scary but rarely dangerous Back pain, if bad enough can disrupt your whole life, it can stop you from working, socialising and exercising therefore has a more profound impact on your life than just physical pain. That’s scary stuff! But the good thing is that even though it is scary and maybe very painful it is rarely dangerous or life threatening. The statistics are only 1-2% of back pain is of a serious pathology that requires immediate attention from the GP or specialist. So yes it does happen but it is very very rare. Fact number 2: Getting older is not a cause of back pain Widely common belief that getting older is a cause of back pain and that if you have back pain, it will only get worse as you age. This is not backed by research and you can certainly recover and manage back pain at any age of life.  Fact number 3: Persistent back pain is rarely associated with serious tissue damage The large amount of research around pain sciences now has helped us understand persistent pain. The human body is strong, and when we do have an injury, tissue healing will occur and generally occur within the first 3 months of the injury. If pain persists past this time it may mean there are other contributing influences such as poor sleep, nutrition, overall health and stress, anxiety or worry. Fact number 4: Scans rarely show the cause of damage Scans are an outstanding bit of technology in which we would be nowhere near where we are today without. Unfortunately scans can tell us lots of scary sounding things but can't actually tell what is the cause of pain or how much pain should be felt. Scans also don't tell us that people without pain can have these scary sounding things as well. Scans are great and necessary but for a smaller number of people. Fact number 5: Pain with exercise and movement does not mean you are causing harm This one is a simple one for me, movement and exercise is one of the best ways to manage and treat low back pain. When people have persistent pain, over time their body will become sensitive to movement and therefore exercise, this however does not mean you are causing harm, it just reflects how sensitive you are. Exercise is again one of the best ways to improve this sensitivity and should be done with a gradual approach. Finding something you enjoy and will consistently do is the key. Fact number 6: Back pain is not caused by poor posture The way you sit at your desk, bend to pick something up or stand around has not been shown to cause back pain. Although certain postures may be painful at times, this does not mean they are the cause of pain. The key to posture is variety, not staying in one position too long. Below I am sitting in all different types of posture which are okay to do but not for too long! Fact number 7: Back pain is not caused by a weak core Hands up if you have heard you need to strengthen your core because you have back pain? This is widely thought and recommended. Yes a strong core is important for human movement and having strong core muscles when we need them is really important. However for many people with low back pain the core muscles are often overactive and cause a tight tense feeling. This is not helpful. Learning to have your core muscles engage when you need them and relax when you don't can be really helpful. Fact number 8: Backs do not wear out with every day loading and bending Everyday loading of the back through bending, twisting and lifting is actually really good for the back and makes you stronger and healthier, just like lifting weights does. However, also like lifting weights, it is important you practice regularly, start and progress slowly and don’t do much more than your current capacity. Fact number 9: Pain flare ups do not mean you are damaging yourself
Flaring up pain can be a scary time however this generally does not mean more damage or a re-injury. Preventing factors such as your overall health (sleep, stress, mood, thoughts and emotions) Staying calm, positive and continuing to move as much as tolerable during a pain flare up is the key to successfully managing back pain flare ups. Fact number 10: Injections, surgery and strong drugs are usually not a cure Some commonly used treatment methods such as injections, surgery and strong drugs can be beneficial for short term gain however they aren’t that effective long term and can actually come with some harmful side effects. Of course everyone is an individual and everyone's back pain is different however these 10 facts are a great start in understanding back pain and getting you moving. Online there is a great resource that can get you started, you can hear from people with lived experience of back pain and how they have managed and overcome this pain. Link: http://www.pain-ed.com/public/patient-stories-2 As always, if you do have any questions regarding this blog please don't hesitate to ask. Izaac Boylan Accredited Exercise Physiologist  With the Aussie rules football season just around the corner, how many of you have committed fully to your pre-season training? Has your pre-season training been sufficient for you to be fully prepared for the physical demands and rigours of playing football? It does not matter your skill level or grade you play you should always prepare well to prevent injury and optimise performance. What physical attributes do you need in football?  Aussie rules football is a unique game. It is a high contact sport which requires a certain amount of physical fitness to perform successfully. The main pillars of physical fitness that the good football players have are:
Injury prevention  Injuries are a big factor in football especially early on in the season. Injuries can make any season into a bad season for a player or a team and it is something you want to avoid. One of the main points for injury prevention is to make sure you are prepared to perform the specific demands of football especially early in the season. If you ask any person playing the game they will tell you the first game or two of the season are the hardest physically. Adequate warm up, good nutrition, good sleep/rest and a good recovery are all part of injury prevention around training and game time. What about during training? We can use something called specificity. Specificity is a term used in exercise science and it means to train the skill/ attribute/ movement you want to perform. You want to use specificity in your football training, particularly at the end of preseason, to best prepare. How to train the main attributes? Aerobic/ anaerobic endurance This one is probably an easy one for most people. Running in football is a non negotiable, so running during training is a must. To be more specific in your running training you need complete continuous running, interval running and short burst running as you do in a game. Elite players can run up to 15km - 18 kms per game so training to at least 6km-10kms a training session will better prepare you. Strength  You need strength to lay tackles, wrestle with opponents, push off opponents and stand your ground when someone is trying to push you. In order to prepare for a game of football fundamental strength of the lower body and core is really important but also discount the benefits of having good upper body strength. This strength can be built using resistance training either in the gym or outside, I won’t get into the specific exercises that you can do. However, in order to be good at tackling and pushing off your opponent, one on one competitive type of training has to happen before the season. Agility  To evade tackles, break tackles or tackle someone on the move, agility is important. To train this specifically you can use drills that incorporate competitive exercises where you're evading another player but you can also do this on your own. Great drills you can do on your own to improve agility all incorporate running at speed and changing direction. You can simply lay cones on the ground in a pattern that requires you to change direction. I would advise using both methods and doing it in multiple directions as football is a 360 degree sport. Speed I think everyone underestimates high speed running and what high speed running actually is. I believe high speed running is a really important factor to train to prevent injuries. In a game of football it is not uncommon to reach top speed because we aren't thinking about it, we’re just playing football, however at training it is different, there is no pressure, no urgency. High speed running should be implemented into any training program. It can be incorporated into your sprinting intervals or can be done separately. I believe it is always good to find what your max speed is and try to hit that at training. Hand and eye/ foot and eye coordination  Coordination is quite common practice at training for any football team, it is just skills training, however there seems to be a misconception that you don't need to bring out the footballs during preseason and preseason should be just running.
Marking, hand balling and kicking are all fundamental skills needed in football and should be practiced whenever you are at football training. If you can’t kick, handball or mark a football as precise as you can or should be able too, your output on the field will be much less! Bottom line in any football preseason is that you need to be training the way you play and not leave it until 2 weeks out from the season. This does not mean all the time and every training but if you don't train at high speeds, have enough specific strength or have enough endurance you will increase your risk of injury during the season. If you want to help better your chances of staying injury free and playing to your potential in the up and coming season, we can help you with some advice, programming or one on one exercise sessions. Izaac Boylan Accredited Exercise Physiologist What is the Tricep muscle? The tricep muscle sits in the back portion of your upper arm, between your elbow and shoulder joints. The muscle is made up of three muscle heads, hence “tri” in the name. Each of the three heads, the long head, medial head and lateral head, play a different role in each movement that it produces. The long head of the muscle is located on the inside portion of the arm, whilst the lateral head sits on the outside and the medical head is positioned between the two. It is surprising that the triceps actually accounts for two thirds of the muscle mass in the upper arm. 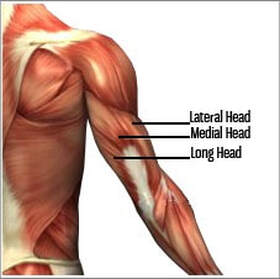 What does the Tricep muscle do? The Tricep’s main function is to assist in stabilising the shoulder joint. It produces elbow extension (straightening out the elbow), shoulder extension (pulling the arm back) and adducts the shoulder (bringing the arm in towards the body). What are the best exercises to work each head of the Tricep? Lateral head: Tricep dips are a fantastic triceps exercise that can be both progressed and regressed depending on your level of ability. They focus on working the lateral head of the tricep but also target the medial and long head too.
Medial head: Overhead tricep extensions are another versatile exercise that can be done seated or standing. Whilst this exercise only uses one dumbbell it is important that you have a good grip with both hands on the dumbbell to ensure it is completed safely.
Long Head: Tricep pulldown with a neutral grip target the long head of triceps but altering the grip position can change the dominant head of the tricep that is working too. This exercise can be done using a cable machine or resistance band at home.
Written by, Aleisha Michael Accredited Exercise Physiologist. |
AuthorSLisa Parkinson Archives
March 2024
Categories
All
|
 RSS Feed
RSS Feed